If the mother already has a balanced diet meeting the RDIs of all essential nutrients prior to pregnancy, only minimal dietary changes are required to ensure she is getting all the nutrients required to sustain a healthy pregnancy. Particularly, calcium, iron and folate intake should be increased. During the later stages of pregnancy calcium intake becomes more important as the babies soft bones begin to mineralise and its muscles begin to contract as it moves about in the uterus. Iron intake also becomes increasingly important to support the increasing oxygen demand of the growing foetus and the mother, whose body is also growing. Late in pregnancy the woman must get sufficient iron to reduce her risk of post-partum haemorrhage and to combat the heavy blood loss in the days and weeks after delivery. The baby also needs adequate iron stores in their body to last for the first 6 months or so of life. Folate is most important in the first trimester of pregnancy.
Different nutrients have different functions in pregnancy. Although many are not required in amounts additional to the RDI for a non-pregnant adult woman, problems arise because most non-pregnant adult women are deficient in some nutrients in the first place. Below is a table explaining some nutrients and how they are important for developing foetuses.
| Nutrient | Recommended Intake | Role in foetal development |
| Calcium | 1000-1300mg | Bone and tooth development, nerve, muscle and heart development and function, blood clotting |
| Chromium | 30mcg | Regulates blood sugar levels, important for tissue formation because it stimulates protein synthesis |
| Copper | 1mg | Development of the cardiovascular, skeletal and nervous systems |
| Fluoride | 3mg | Crucial for tooth formation which starts in the first trimester and continues throughout the remainder of pregnancy |
| Folate/Folic Acid | 600-800mcg especially in the first trimester, 400mcg pre-conception | Proper development and closure of the spinal cord and canal from the neural crest early in pregnancy. Important for DNA synthesis and brain function |
| Iodine | 220mcg | Nervous system development (deficiency in pregnancy strongly linked to cretonism in children) and also important for metabolic regulation |
| Iron | 30mcg | Particularly important in second and third trimesters for oxygen supply and subsequent energy production required to fuel growth, important for bone formation |
| Magnesium | 350mg | Bone and tooth development, blood sugar regulation and tissue growth |
| Manganese | 2mg | Important in bone mineralisation, and also in pancreatic development and metabolism of fats and carbohydrates |
| Pantothenic Acid | safe limit 6mg
(no set RDI) |
Important for adrenal function, metabolism and also immune function |
| Phosphorus | 700mg | Important for bone and tooth mineralisation, heart function and blood clotting |
| Potassium | safe limit 2000mg
(no set RDI) |
Important in developing muscles and heart and also for nerve function |
| Riboflavin | 1.4mg | Required for proper growth and also development of a variety of tissues including the skin. Important for good vision. |
| Thiamine | 1.4mg | Very important for carbohydrate metabolism and brain development. Also important for the developing heart and nervous system |
| Vitamin A | 2500IU | Important for the development of mucous membranes and the eyes as well as immune system development |
| Vitamin B6 | 1.9mg | Important for metabolism and energy production, also needed for production of new blood cells and heart and nervous system development |
| Vitamin B12 | 4-6mcg | Important for metabolism and energy production, for red blood cell production and nerve development |
| Vitamin C | 60-70mg | Crucial for immune function, collagen production, bone and tooth development and tissue repair. Important in pregnant women with substance abuse problems or who smoke for protection of the foetus from toxins and free radicals |
| Vitamin D | 400IU | Most important function is in bone and teeth development, aids in absorption of calcium also |
| Zinc | 11mg | Very important for cell division and tissue development |
Caloric Intake in Pregnancy
One of the most common myths surrounding pregnancy is that a woman must eat for two. While it is true that she is supplying all the growing baby’s nutrients, for the majority of the pregnancy, the growing baby is tiny. Early pregnancy is characterised by development and maturation of tissues, organs and body systems, it is only in the latter stages of pregnancy that significantly growth in length and weight really occur. A 1lb, or 0.5kg foetus certainly does not need the same amount of calories as a fully grown adult!
A pregnant woman of average physical fitness and activity levels will need only a moderate increase in her daily calorie intake. The first trimester should see a woman consuming a similar amount of calories as she was pre-pregnancy. The foetus at this stage is tiny and the mother, although her body is changing will not need much extra calories yet. By the second trimester, after the placenta has formed and the mothers’ body is changing more rapidly and blood flow and supply is increasing, approximately 300 calories extra per day will be needed to meet energy requirements. For athletic women up to 500 calories extra may be needed.
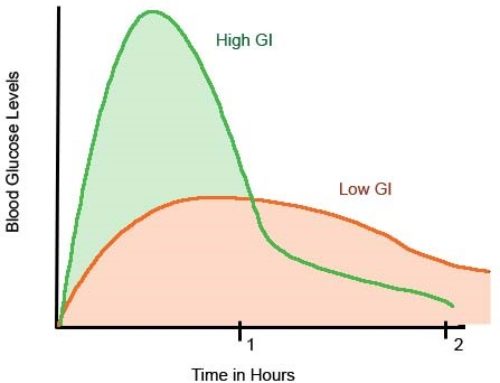
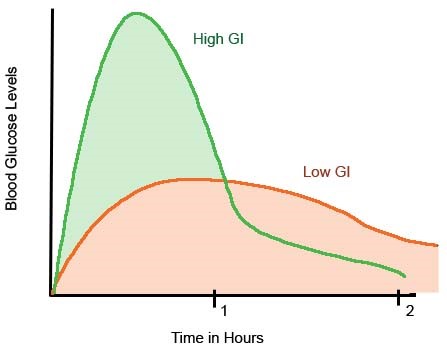
While a moderate increase in caloric intake is important, more important is the source of the additional calories. Pregnancy can leave a woman less sensitive to insulin than normal, meaning she is less able to cope with the fluctuations in blood sugar levels brought on by simple sugars. Calories should not be sourced from foods that are not also rich in other essential nutrients. Empty calories from fast foods, sweets and junk food are not recommended, instead, fruits and dairy, which contain sugars (fructose and lactose respectively) that do not cause such dramatic changes in blood sugar as glucose and sucrose, and which also contain a variety of other important nutrients, make excellent calorie sources.
Course Extract from the Children’s Nutrition course run by Health Academy Australia

{kind=link}
{kind=link}
{kind=link}
Leave A Comment